Founded December 2025 · Seoul, Korea
Targeting the
Impossible
TAREXIS discovers novel First-in-Class anticancer targets through real-world patient data — bridging the translational gap with Tx-Finder™ and Tx-Verifier™.
FIC Antibody-based Anticancer Therapeutics · Real-World Evidence Driven Discovery Platform
6+
FIC Programs
$58B
NSCLC Market 2028E
3R
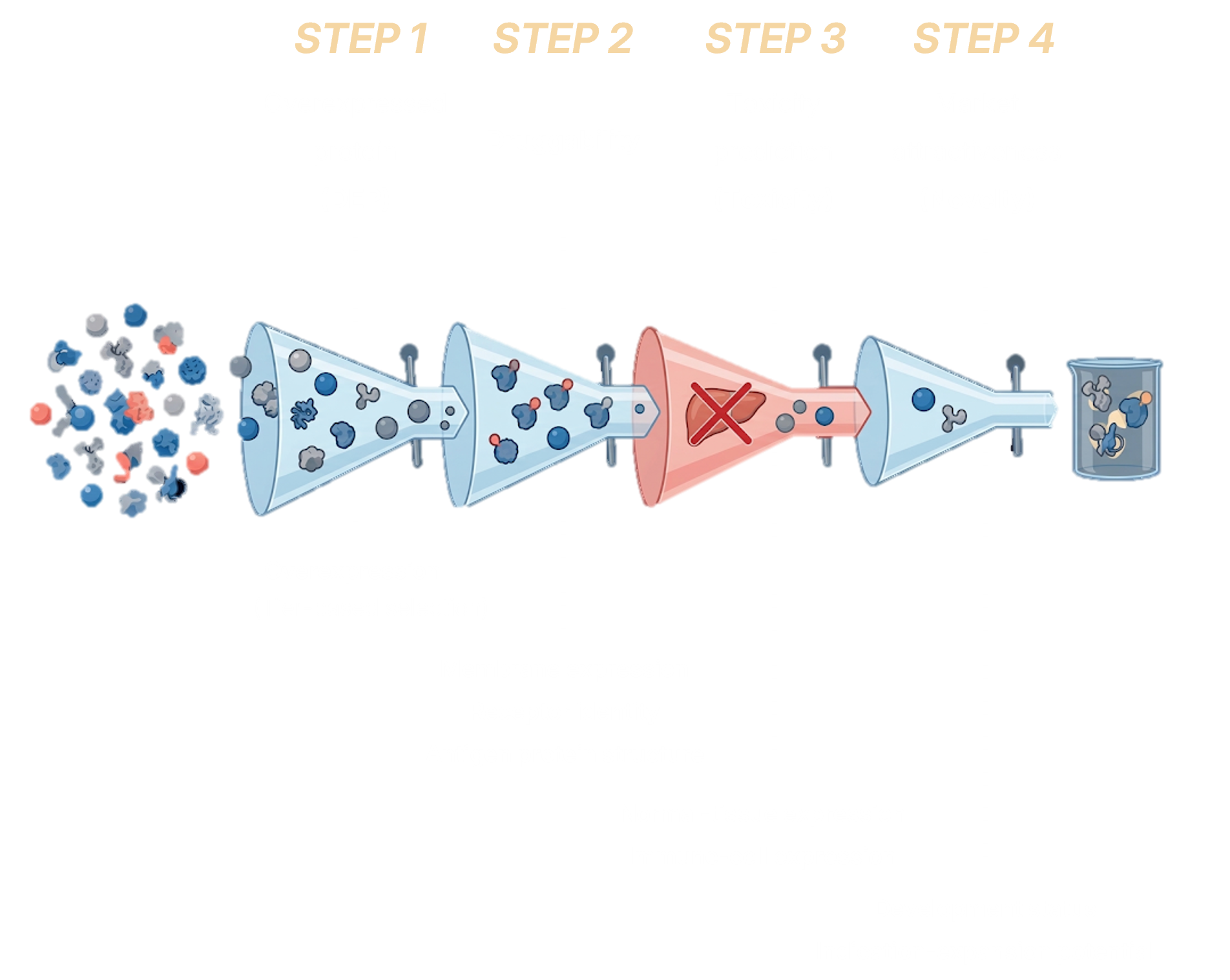
Discovery Framework
2
Global Partners
Scroll